
Wire-In-Needle (WIN) Technique for Ultrasound-Guided Central Venous Catheterization
We all learned to place central lines in the same way: use a finder needle, aspirate blood, thread the wire, dilate, place your line. It works! It’s reliable, safe, and easy. So why learn a new technique for a procedure we are already pretty good at? Because ultrasound changes the game (again). Rather than use ultrasound as just an adjunct to an old method, we advocate letting it change the procedure itself – eliminating obsolete steps for a more efficient, reliable and safe procedure.
Here, we introduce the “Wire-In-Needle” (aka the “WIN” or “syringe-free” technique) for ultrasound-guided central venous catheter placement.(1) With the traditional Seldinger technique, after aspirating blood from the finder needle, the syringe is detached and the wire is threaded into the vein. As anyone who has placed a central line knows, this is one of the most error-prone steps because after removing the syringe, the finder needle can be accidentally displaced such that the wire will no longer thread into the lumen of the vein. With the WIN technique, which we first learned about from Mike Stone, the wire is inserted inside the finder needle prior to skin puncture and ultrasound is used for direct, real-time visualization of the guide wire entering the vessel.(2)
Watch the video!
Procedure overview:
- Setup: Use a standard central-line insertion kit. Instead of attaching the syringe to the finder needle, insert the wire directly into the needle, until the J-tip is just proximal to the end of the needle. The syringe is not used. If needed, use sterile scissors to shorten the tapered end of the wire spool, such that it fits snugly into the needle (this may not be indicated in all kits).
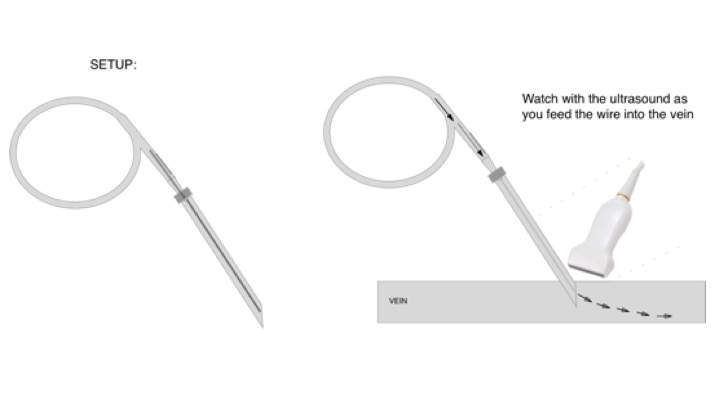
- “Syringe-free” vessel cannulation: Using ultrasound guidance in either short- or long-axis, insert the finder needle into the vessel. With the ultrasound in long-axis view of the vein, advance the wire through the needle tip and watch as the J-tip enters the vessel. Remove the needle, leaving the wire in place.
- Safety check: Confirm that the wire is in the vein, by tracking it to the back wall of the vessel and using proximal pressure to ‘bounce’ the wire while watching it on ultrasound.
- Finishing: Now proceed with central line insertion as with the traditional technique, including vessel dilation and inserting the catheter over the wire.
Procedure step-by-step:
- Identify best CVC site (internal jugular, supraclavicular, infraclavicular, femoral) given patient factors including anatomy and clinical context.
- Use of the Wire-in-Needle (WIN) technique is most appropriate for IJ, supraclavicular and femoral CVC.
- Use ultrasound while selecting CVC site to verify a central vein that is of adequate diameter, is compressible (i.e. no DVT) and does not lie deep to important structures – for example, an internal jugular vein which lies deep to the carotid.
- Position and prepare patient, central line equipment (including ultrasound), in sterile fashion as usual.
- Prepare the needle and wire apparatus
- Place the finder needle over the end of the tapered guide on the wire spool and advance the wire until it emerges from the end of the finder needle, then retract until the tip is fully within the finder needle.
- Optional: use the suturing scissors or scalpel to cut the tapered guide on the wire spool to more snuggly fit the finder needle hub.
- Hold the WIN apparatus in your dominate hand with the “shooter” hand grip such that your index finger provides control of the finder needle while your thumb is positioned to easily advance or retract the wire.
- Find the target vessel on ultrasound in short axis (aka transverse).
- Confirm the vessel is venous by compressing the vein fully and visualizing the accompanying artery pulsate while the collapsed vein does not.
- With the target vessel on the ultrasound midline (in the center of the monitor), slowly rotate the transducer counter clockwise while keeping the vessel in view at all times until the indicator marker is pointed towards you and you are visualizing the central vein in long axis (aka longitudinal).
- Using in-line technique, insert the finder needle at an approximate 30 degree angle directly under the ultrasound probe indicator and parallel to the ultrasound probe orientation.
- Directly visualize the entire shaft and tip of the inserted portion of the needle as you advance the needle and puncture the vein.
- Once the tip of the needle is visualized in the center of the vein in long axis, use your thumb to advance the wire and visualize the emerging J-tip portion of the wire into the lumen of the vessel.
- Sufficiently advance the guide wire and keep it in place as you remove the finder needle while always holding on to the guide wire.
- Prior to dilation, confirm correct guide wire placement with ultrasound:
- In short axis, visualize the guide wire entering the lumen of the vessel
- For internal jugular and femoral veins, compress the vessel containing the guide wire to confirm that the wire is in the vein and not the artery
- For supraclavicular approach to subclavian vein, use Doppler to confirm that the vessel containing the guide wire has venous pattern of flow (vs arterial).
- If guide wire is resting against wall of vein, “bounce” the wire to confirm that it is not, in fact, through-and-through the vein. While visualizing the wire against the wall of the vein, place your finger over the wire’s point of insertion into the skin and press down into the soft tissue. This should cause the wire to “bounce” away from the wall, proving that it is intraluminal and not through-and-through.
- Continue with usual central line insertion technique including nicking the skin, dilating, inserting the central venous catheter, removing the wire, ensuring adequate flow and blood return, and properly securing and dressing the site.
Have you tried this technique? Any concerns about using it? Leave your feedback on this post!
Citations:
(1) Ince et al. Comparison of transverse short-axis classic and oblique long-axis “Syringe-Free” approaches for internal jugular venous catheterization under ultrasound guidance. Rev Bras Anestesiol. 2018 Feb 22.
(2) Stone, M. Another WIN for Ultrasound: the Wire In Needle technique for CVC Placement. https://vimeo.com/57077000 Accessed 5/18/2018.
Other resources:
Ultrasound Podcast Wire in Needle Technique
EMCRIT Podcast 156 – The Central Line Show – Part I: Avoiding Complications


October 28, 2020 at 12:00 am
With a standard J-wire I’ve found this to be pretty safe. Using a micropuncture (0.018″) wire, I have twice had the wire migrate ahead of the needle. This was despite “being careful” not to the second time. Should I try it again, I may clamp the wire with the needle driver at the needle hub. Adding a Touhy-Borst valve would work too. But all that movement, you may as well have the syringe on.
I could see a novice accidentally advancing the wire too soon with a larger wire. Unrecognized, it could get messy…. Good long axis on the needle technique is your best insurance, but depending on the resolution of the US machine, the microwire tips can be tough to see, even on long axis, since they are thin and floppy.
LikeLike
April 21, 2021 at 1:35 am
At what stage do you confirm venous placement with manometry? Ultrasound use alone doesn’t guarantee venous placement. I have seen many a resident go through the vein into the artery without realizing it even with decent ultrasound skills.
LikeLike